Travelling with Crohn's Disease
Last Updated: 22/04/2024
For patients who travel with Crohn's disease, there are some issues to consider that are unique to Crohn's disease and are rarely a concern for patients with ulcerative colitis. This page will address travel-related issues for Crohn's disease patients. Other important information for travel including diet, insurance, vaccinations and more, can be found in the section on 'Travelling with IBD'
Travelling with perianal Crohn’s disease.
If you are a Crohn's disease patient with known perianal disease, either having a perianal fistula and/or if you have had perianal abscess in the past, you should take precautions to reduce the risk of a perianal abscess occurring during travel, as this may require urgent medical and/or surgical treatment.
Learn more about healthcare abroad.
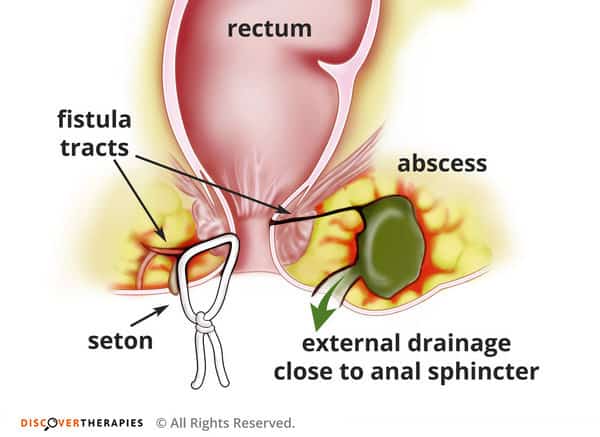
Image showing how perianal Crohn’s can occur, including abscess formation and seton insertion
These precautions include:
- In general, if you have occasional pain in the perianal (buttock) region, it is advisable to be checked by your IBD team before the trip to decide if a collection of pus (a small abscess) is the cause of pain. This is usually diagnosed by an MRI scan of the area or in severe cases by an examination under anesthetic by a colorectal surgeon.
If you are found to have an abscess, it may need to be treated with either antibiotics or, if it is severe, surgery to drain it. Seton draining strings such as that shown in the image are often used to prevent an abscess returning and are usually in place for a few months. They should not prevent you from physical activity including swimming or bathing during travel, and are helpful in reducing the risk of recurrent abscess during travel.
- If you have occasional or constant discharge from a perianal fistula, ask your doctor for antibiotics such as ciprofloxacin and metronidazole. These can often be used for up to two weeks or sometimes longer to reduce the amount of discharge or if the discharge increases in amount and causes excessive discomfort. Depending on the amount of discharge you experience, you may want to consider also to have in your carry-on luggage an adequate supply of sanitary pads, and additional pair of underwear.
- If you have or previously had a perianal fissure (A small tear in the anal area sometimes caused by frequent toilet visits or passing hard stool) then consider taking with you a specialized cream for local application to alleviate the pain and hasten the healing. Creams such nifedipine 0.2% or nitroglycerine cream are available and can be prescribed by your doctor. Be aware that these creams may need to be taken in the luggage and not in the carry-on bag if their volume exceeds 50-100cc (100ml), depending on specific airport regulations. A letter can be obtained from your doctor or IBD team stating your need for this cream will sometimes help in passing through security. It is always advisable to enquire with the airline or airport beforehand for specific airport regulations regarding travelling with medications.
If you are planning to travel with medication, then refer to our 'Travel with Medication' for further advice
Image showing perianal fissure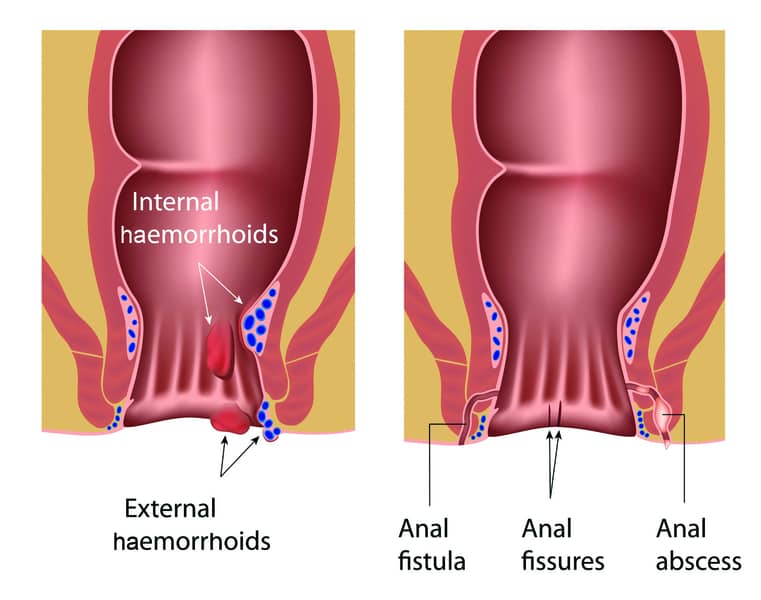
Intestinal strictures and bowel obstruction
Some Crohn’s disease patients may have stenosis or strictures (narrowing) of the intestine, in particular the small intestine. This can cause bloating and abdominal distention after eating, pain, nausea and even vomiting if obstruction to intestinal flow is severe. If you know you have or have had a stricture (narrowing) in your bowel, it is advisable to exercise extra-caution in consumption of fiber-containing food. Specifically, raw vegetables and fruits, but also popcorn, sunflower seeds and swallowing chewing gums should be refrained from or consumed only carefully during the trip. If you do experience the onset of pain and bloatness during the trip, unaccompanied with diarrhea, this may indicate the beginning of a bowel obstruction. Seek medical advice, but if this is not readily available, try to avoid solid food for 24 hours and consume only fluids and/or nutritional formulas if tolerated until medical assessment can be arranged. A severe onset of pain accompanied with fever, rigors or vomiting should always prompt urgent medical assessment.

Nutritional support
Crohn’s disease patients are often in need for nutritional support to offset deficiencies in calories or in important nutritional components such as proteins or vitamins. It is advisable to have pre-travel assessment of your nutritional status with your IBD clinic or Dietician and to correct any deficiencies such as in protein levels or vitamin B12 or iron stores, especially if you plan a long-term trip.
If you are already receiving regular oral nutritional support in the form of oral formulas, you will have to ensure that these are available for purchase in your destination country as it is often hard to carry enough of these during travel. Powder form nutrition may be easier to take in your luggage and supplement your needs for longer than liquid based formulas. Consult your dietician before travel
If you are receiving Total parenteral nutrition intravenously, then refer to our Diet webpage for further advice